A 16-year-old boy named Roger lay sick in his bed, week after week, recovering from his second serious bout of Nephritis (kidney inflammation).
Long stretches of fatigue and immobility. He’d already cycled through hospital stays for it. Gloomy ones, by his own description. But at home, in his bedroom, he had a window. And out that window was a single big pine tree.
He stared at it a lot. There wasn’t much else to do.
He came out of it fine. His kidneys recovered. Years later, he’d say that tree helped his emotional state immensely. Just having something alive in his line of sight, day after day, made the long sick stretches more bearable.
In grad school, he found a field that let him study the experience he had as a teen more deeply. Environmental aesthetics. The basic science of whether the beauty of the living environment mattered to the human nervous system. He started with a question.
Which groups of people experience a lot of emotional duress and might benefit from a view of nature?
Hospital patients and prisoners.
So he designed a study to analyze his hunch, and in April of 1984, Dr. Roger Ulrich published a paper in Science magazine called “View Through a Window May Influence Recovery from Surgery.” It is, by most accounts, the single most influential study in the history of healthcare architecture. And even launched an entire field called evidence-based design.
And the design of the study itself is almost as interesting as the findings. Let me walk you through it.
The study.
Ulrich’s hypothesis was simple. A hospital window view of nature should help patients recover from surgery faster than a view of a wall.
This was a retrospective records review.
The setting was Paoli Memorial Hospital, a 200-bed facility outside Philadelphia. It had a quirk that made it nearly perfect for this kind of study. There was a three-story wing where windows on one side looked out at a small stand of trees, and windows on the other side looked out at a brown brick wall. The rooms on both sides were nearly identical (same dimensions, same window size, same furniture arrangement). The same nurses cared for patients on both views. Patients were assigned to rooms as they became vacant. Essentially random with respect to view.
In other words, every gallbladder surgery between 1972 and 1981 at this hospital had been an unintentional little experiment. Ulrich just had to find the records and analyze them.
He pulled them, then filtered:
- Same surgery. Only cholecystectomy (gallbladder removal) patients. Different procedures recover differently.
- Same time of year. Only surgeries between May 1 and October 20. This is when the trees outside had full foliage. He didn’t want bare winter branches watering down the “tree view” condition.
- Same age range. Only patients 20 to 69, to remove confounders related to age-driven recovery differences.
- No serious complications. No psychiatric history. Anyone whose recovery would be skewed by other factors got cut from the analysis.
What was left were 46 patients. He matched them into 23 pairs (one tree-view, one wall-view per pair), controlling for sex, age, smoking status, body weight, year of surgery, and floor. He even matched the room color, where the rooms on the second floor alternated between blue and green. Then he had a nurse with surgical floor experience extract the recovery data from the records.
Three primary outcomes he tracked:
- Length of postoperative hospital stay.
- Pain medication intake, broken down by potency (strong narcotics, moderate analgesics, weak analgesics).
- Nurses’ notes, scored for negative comments (”upset and crying,” “needs much encouragement”) versus positive ones (”in good spirits,” “moving well”).
The findings are all in favor of the tree-view group
- Shorter hospital stays. 7.96 days versus 8.70 days on average. Statistically significant.
- Less powerful pain medication. During days 2 through 5 after surgery (the period when patients are alert enough to actually engage with their environment), wall-view patients received many more doses of strong narcotics like Dilaudid. The tree-view group stepped down to weaker meds (aspirin, acetaminophen, codeine) sooner.
- Far fewer negative nurses’ notes. This is the wildest stat in the paper. Wall-view patients averaged 3.96 negative comments per chart. Tree-view patients averaged 1.13. About four times the volume of negative observations from the same nursing staff who couldn’t even see the view themselves.
Wow!
Forty years later, the paper has been cited thousands of times. Multiple research groups have independently replicated the core finding using different patient populations and outcome measures. And the modern hospital design industry, which spends billions of dollars a year on new construction, treats “what can the patient see?” as a first-order design constraint.
The rise of “biophilic” design.
Ulrich’s 1984 study didn’t invent the idea of nature in healthcare. But it was the first time the effect had been measured rigorously enough to convince hospital administrators and architects that it actually mattered.
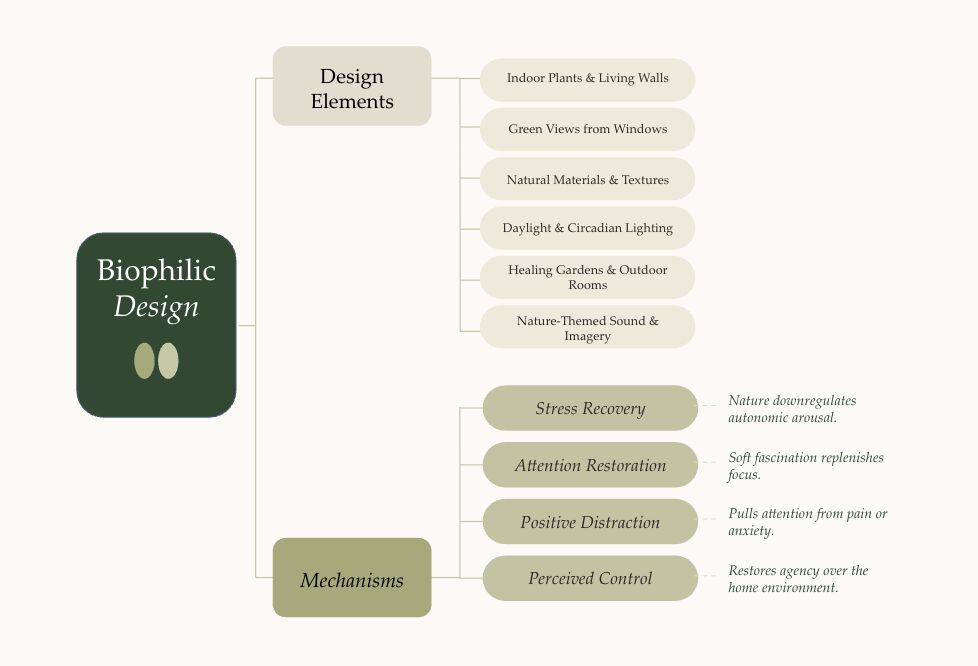
Out of that paper, and the decades of follow-up research it spawned, came an entire design movement called biophilic design. The premise is that humans evolved in nature, our nervous systems are tuned to it, and intentionally designing buildings to integrate natural elements has measurable effects on the people inside them.
A 2026 rapid review in Frontiers in Public Health synthesized the evidence on biophilic interventions across hospitals worldwide. The interventions:
- Indoor plants in patient rooms, lobbies, and corridors
- Green views from hospital windows (Ulrich’s original variable)
- Natural materials like wood, stone, and plant-based panels
- Daylight optimization through skylights, larger windows, and orientation
- Healing gardens and accessible courtyards
- Nature-themed digital media, from murals to projected landscapes to VR
The findings, across dozens of studies, were consistent. Patients exposed to these elements showed lower stress, less anxiety, better sleep, reduced pain medication use, faster emotional recovery, and higher satisfaction with their care.
The strongest effects came from direct exposure to real nature. Simulated nature (digital forests, VR experiences) worked too, just less powerfully. Static nature imagery worked least, but still measurably. Researchers call this a dose-fidelity gradient: the more real the nature, the bigger the effect. (More on this below.)
Four ways a space can actually heal you.
A recent study, March 2026, has identified four mechanisms by which nature-integrated design influences patient outcomes. This is the part I find most useful, because it’s not really about hospitals. It’s about how human nervous systems respond to the spaces we put them in.
Stress recovery. Natural elements downregulate the autonomic nervous system. Heart rate drops. Cortisol drops. Heart rate variability improves (a marker of parasympathetic activity, the “rest and digest” mode). The body shifts out of fight-or-flight.
Attention restoration. Modern life requires constant directed attention (screens, decisions, traffic, deadlines), and that capacity gets depleted. Nature engages what they call soft fascination: the brain finds it interesting without effort. That low-effort engagement lets directed attention recover.
Perceived control. When patients have access to a window, a garden, or even just a view, they feel less helpless. The same goes for adjustable lighting, choice of room layout, or being able to open a window. Loss of control is one of the most stressful aspects of being hospitalized. Design that restores some of it has measurable effects on mood and recovery.
Positive distraction. Pain and fear are partially attentional. When attention is captured by something engaging (an aquarium, a garden view, a calming piece of art), the perception of pain drops. There are now multiple randomized controlled trials showing that nature-based distraction reduces post-surgical pain.
For the nerds. Dose-fidelity gradient.
All of this research has shown that there is a hierarchy of effect sizes when it comes to nature exposure in healthcare settings.
- Direct, multisensory contact with real nature (gardens you can walk in, water you can hear, plants you can touch). Strongest effect on stress, mood, and physiological recovery.
- Visual access to real nature (window views, accessible courtyards). Slightly weaker but still robust.
- High-fidelity simulated nature (VR forests, immersive digital environments, dynamic projections). Moderate effect.
- Static nature imagery (photos, murals, framed prints). Smallest measurable effect, but not zero. Better than blank walls.
- No nature exposure. Baseline.
Translation. Fidelity matters, but stacking matters more. A space with real plants, a real window view, natural materials, and daylight will compound across all four mechanisms. A space with one nature mural and fluorescent lighting won’t.
These studies were fun to read and analyze. I am just scrapping the service, more to come.
Hunter
We built a bunch of FREE resources for you!
- Take our home health quiz (~5 min)
- View a recent home assessment report
- Try out our indication guide to lead pipes
- See your radon risk with our Minnesota radon map
- Calculate what the best air purifier is for your home from our database
- Schedule a free 15 minute chat with our founder about any questions you have
.webp)